- About
-
Services
- Eye and Vision Exams
- Comprehensive Eye Exam
- Contact Lens Exams
- Pediatric Eye Exams
- Ocular Disease Management
- Dry Eye
- Lasik Eye Surgery co-management
- Glaucoma
- Cataracts
- Macular Degeneration
- Keratoconus
- Eyeglasses
- Designer Frames
- Picking The Right Frames
- Sunglasses
- Eyeglasses FAQ
- Conditions Treated
- Blurry Vision
- Red Eye
- Itchy & Burning Eye
- Common Injury
- Eye Focusing Problem
- Lazy Eye
- Computer Vision Syndrome
- Emergency Eye Care
- Common Eye Injuries
- Contact Lenses
- Myopia Management
- Dry Eye
- Patient Center

Pediatrician Referral Form

All Eye
Care Services

Keep
In Touch
MAP
CONTACT INFORMATION
HOURS OF OPERATION
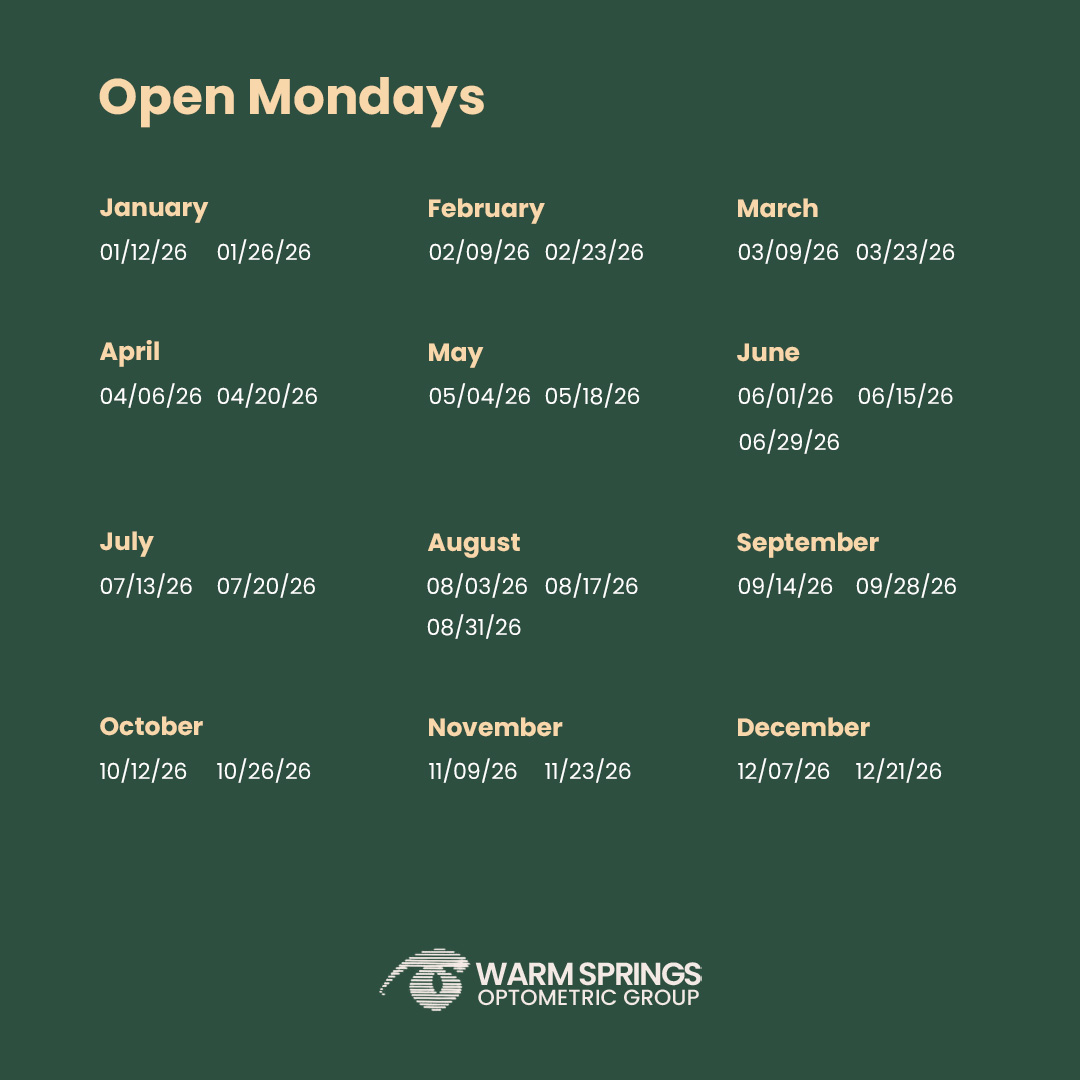
Monday 9:00 AM - 5:00 PM(Alternating Mondays)
Tuesday 9:00 AM - 6:00 PM
Wednesday 9:00 AM - 6:00 PM
Thursday 9:00 AM - 6:00 PM
Friday 9:00 AM - 5:00 PM
Saturday 8:00 AM - 1:00 PM(Alternating Saturdays)
Sunday Closed
Closed for Lunch 1-2 PM
© 2026 Warm Springs Optometric Group. All Rights Reserved. Accessibility Statement - Privacy Policy - Sitemap
Powered by: